

Introduction
Relapses involving the central nervous system (CNSrel) occur in ~5% of patients (pts) with aggressive non-Hodgkin lymphoma (NHL) in the rituximab era (Ghose et al, Clin LML 2015) with rates exceeding 10% in high risk groups (Villa et al, Ann Onc 2010; Schmitz et al, JCO 2016). CNSrel are generally thought to occur in the first 4-6 months from diagnosis. Prophylaxis (PPx) administration, route, and frequency are not standardized, and the impact of PPx on CNSrel risk is incompletely understood.
Methods
We performed a multicenter retrospective analysis of pts with aggressive NHL (excluding Burkitt's) without known CNS involvement (inv) who received single-route CNS PPx with during front-line (FL) anthracycline-based therapy (tx) from 2013-2019 across 19 US academic institutions. Recipients of chemotherapy for prior CLL or indolent NHL were ineligible. Method, frequency, and outcomes of CNS PPx administration were evaluated, with significance assessed by various statistical methods via two-tailed P<0.05.
Results
1030 patients were identified who met eligibility criteria. Clinical features included median age 61 years (yrs; range 16-86), 40.9% female, ECOG PS 0-1 82.8%, elevated LDH 65.3%, >1 extranodal (EN) site 42.3%, stage 3/4 disease 79.2%. NHL histologies included diffuse large B cell (DLBCL; 75.2%), high grade B cell (16.3%), transformed follicular lymphoma (5.6%) and 3% other; among pts with DLBCL, 46.4% had germinal center (GCB) subtype and 40.5% had non-GCB. 26.2% (n=210) of evaluable pts had double-hit lymphoma (DHL). Among pts with known HIV status, 7.2% (n=65) were HIV-positive. 85.7% had EN inv; common sites included bone (35.4%), liver (13.7%), gastrointestinal (12.7%), lung (11.8%), and marrow (11.5%).
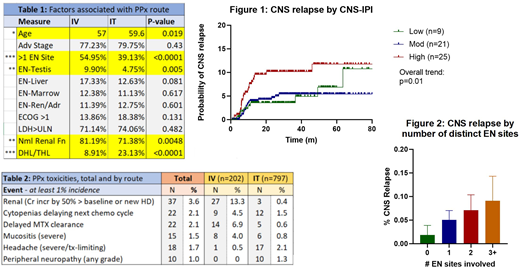
FL regimens included RCHOP (45.9%), REPOCH (46.5% total; 79.1% with dose-adjustment), 7.6% other. PPx was given intravenously (IV) in 20% of pts vs 77% intrathecally (IT), over a median 2.9 vs 4.1 doses respectively; see Table 1 for factors associated with PPx route. PPx was generally well-tolerated, with 10.7% PPx-related toxicity reported; see Table 2.
CNSrel after FL tx was 5.3% overall without significant difference by PPx route (7% IV vs 5% IT, p=0.178). This lack of difference between PPx routes was observed in all subgroup analyses performed, including by: age, stage, histology, number of EN sites, individual EN site inv, elevated LDH, CNS-IPI, DHL status, HIV status, FL regimen, number of PPx doses. There was no significant difference in anatomic site(s) of CNSrel by PPx route.
CNSrel occurred bimodally: 24% by end of FL tx vs 76% delayed (average 2.3 yrs, range 0.4-5.2 yrs). Rates of CNSrel were significantly higher with CNS-IPI high vs moderate risk (8.3 vs 4.1%, p=0.03; Figure 1), elevated LDH (6.9 vs 2.6%, p=0.007) and multiple inv EN sites (7.5% for 2+ vs 4% for 0-1, p=0.01); each additional EN site further increased risk (p=0.03 for trend; Figure 2). Increased CNSrel was noted in pts with testis (13.7 vs 5%, p=0.004) and liver inv (11.1 vs 4.6%, p=0.002) vs those without inv at respective sites. No significant difference was noted at other EN sites, including renal/adrenal (4.8 vs 5.6%, p=0.71), marrow (8.9 vs 5.1%, p=0.09), or lung (8.6 vs 5.1%, p=0.12). All EN site-CNSrel correlations were unchanged when accounting for PPx route.
With median follow-up of 2.3 yrs, median PFS and OS for the overall group have not been reached; 2-yr PFS and OS were 70 and 85% respectively. PFS and OS were each predicted by CNS-IPI (p<0.0001) and maintained significance when separated by PPx route. 196 deaths were reported, including 122 disease-related and 34 tx-related (TRM). There was no significant difference in TRM by PPx route (1.9% IV vs 3.6% IT, p=0.24). Death due to progression was more common following IT PPx (13.3% vs 7.9% IV; HR 1.72, p=0.04), driven primarily by DH status (adjusted PPx HR: 1.54, p=0.11). In those with CNSrel, subsequent relapse and/or death was common (n=41, 74.5%) regardless of initial PPx route or salvage tx. Median survival after CNSrel diagnosis was poor (7.1 months, range 1 day-5.3 yrs) and was significantly inferior to those with non-CNSrel (HR 1.488, p=0.03).
Conclusion
Use of single-route ppx demonstrated similar CNSrel vs established outcomes for this population in the rituximab era, with no difference by PPx route. CNSrel remains a rare but devastating complication, with greater risk even after single-route PPx in those with higher EN burden and inv of key EN sites.
Kahl:Acerta: Consultancy, Research Funding; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees; ADC Therapeutics: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; BeiGene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche Laboratories Inc: Consultancy; Pharmacyclics LLC: Consultancy; Genentech: Consultancy; Celgene Corporation: Consultancy; AstraZeneca Pharmaceuticals LP: Consultancy, Membership on an entity's Board of Directors or advisory committees; AbbVie: Consultancy. Spinner:Notable Labs: Honoraria. Advani:Celgene, Forty Seven, Inc., Genentech/Roche, Janssen Pharmaceutical, Kura, Merck, Millenium, Pharmacyclics, Regeneron, Seattle Genetics: Research Funding; Astra Zeneca, Bayer Healthcare Pharmaceuticals, Cell Medica, Celgene, Genentech/Roche, Gilead, KitePharma, Kyowa, Portola Pharmaceuticals, Sanofi, Seattle Genetics, Takeda: Consultancy. Voorhees:AstraZeneca: Research Funding. Grover:Genentech: Research Funding; Tessa: Consultancy. Huntington:Genentech: Consultancy; Novartis: Consultancy; Celgene: Consultancy, Research Funding; TG Therapeutics: Research Funding; Pharmacyclics: Honoraria; Bayer: Consultancy, Honoraria; DTRM: Research Funding; Astrazeneca: Honoraria; AbbVie: Consultancy. Spurgeon:Beigene: Research Funding; Gilead: Research Funding; Genentech: Research Funding; Bristol-Myers Squibb: Research Funding; Pharmacyclics: Consultancy; Janssen: Consultancy, Research Funding; VelosBio: Consultancy, Research Funding; Cardinal Health: Honoraria; Verastem: Research Funding; Genmab: Research Funding; AstraZeneca: Research Funding; Acerta: Research Funding. Olszewski:Spectrum Pharmaceuticals: Research Funding; Genentech, Inc.: Research Funding; Adaptive Biotechnologies: Research Funding; TG Therapeutics: Research Funding. Landsburg:Seattle Genetics: Speakers Bureau; Morphosys: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Curis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Takeda: Research Funding; Triphase: Research Funding. Kamdar:Roche: Research Funding. Caimi:Kite Pharma: Other: Advisory Board; ADC Therapeutics: Other: Advisory Board, Research Funding; Verastem: Other: Advisory Board; Amgen: Other: Advisory Board; Bayer: Other: Advisory Board; Celgene: Speakers Bureau. Karmali:Takeda: Research Funding; BeiGene: Speakers Bureau; AstraZeneca: Speakers Bureau; Karyopharm: Honoraria; Gilead/Kite: Honoraria, Other, Research Funding, Speakers Bureau; BMS/Celgene/Juno: Honoraria, Other, Research Funding, Speakers Bureau. Stephens:Pharmacyclics: Consultancy; Innate: Consultancy; Verastem: Research Funding; Karyopharm: Consultancy, Research Funding; Janssen: Consultancy; Gilead: Research Funding; Arqule: Research Funding; Juno: Research Funding; MingSight: Research Funding; Acerta: Research Funding; Beigene: Consultancy. Smith:Genentech/Roche: Consultancy, Other: Support of parent study and funding of editorial support, Research Funding; TG Therapeutics: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Janssen: Consultancy; BMS: Consultancy; Karyopharm: Consultancy, Research Funding; FortySeven: Research Funding; Pharmacyclics: Research Funding; Acerta: Research Funding. Khan:Celgene: Research Funding; Pharmacyclics: Honoraria; Seattle Genetics: Research Funding; Bristol Myers Squibb: Research Funding; Janssen: Honoraria. Cohen:Genentech, BMS, Novartis, LAM, BioInvent, LRF, ASH, Astra Zeneca, Seattle Genetics: Research Funding; Janssen, Adicet, Astra Zeneca, Genentech, Aptitude Health, Cellectar, Kite/Gilead, Loxo: Consultancy. Portell:Bayer: Consultancy; Xencor: Research Funding; BeiGene: Consultancy, Research Funding; Infinity: Research Funding; Roche/Genentech: Consultancy, Research Funding; Amgen: Consultancy; Janssen: Consultancy; Pharmacyclics: Consultancy; AbbVie: Research Funding; TG Therapeutics: Research Funding; Kite: Consultancy, Research Funding; Acerta/AstraZeneca: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal